機械通氣的氣道濕化
在正常生理(lǐ)狀态下,吸入氣體(tǐ)通過上呼吸道加溫加濕作(zuò)用(yòng)達到BTPS狀态,即氣體(tǐ)溫度達到37℃, 絕對濕度44mgH2O/L,相對濕度100%。而在正壓通氣或建立人工(gōng)氣道的情況下,呼吸機通過高壓或高流速輸送的氣體(tǐ)較為(wèi)幹燥,使上呼吸道生理(lǐ)性加溫加濕功能(néng)負擔加重,此時,使用(yòng)呼吸濕化器提供足夠的濕化補償就顯得尤為(wèi)必要。

上呼吸道可(kě)以提供吸入氣體(tǐ)75%的濕度。在進行有(yǒu)創機械通氣時,因人工(gōng)氣道的建立,上呼吸道被旁路,不能(néng)對吸入氣體(tǐ)進行加溫加濕時,濕化器就需要補償丢失的這部分(fēn)溫度和濕度。吸入氣體(tǐ)總的濕度需求是44mg/L,被旁路的75%氣道濕化功能(néng)需要濕化器進行補償,即0.75*44mg/L=33mg/L。因此,對有(yǒu)創通氣患者進行主動濕化達到理(lǐ)想BTPS狀态時,濕化器需要提供33-44mg/L 的濕度,對應的氣體(tǐ)溫度在34-41℃之間,相對濕度達100%來維持正常呼吸道的生理(lǐ)功能(néng)。
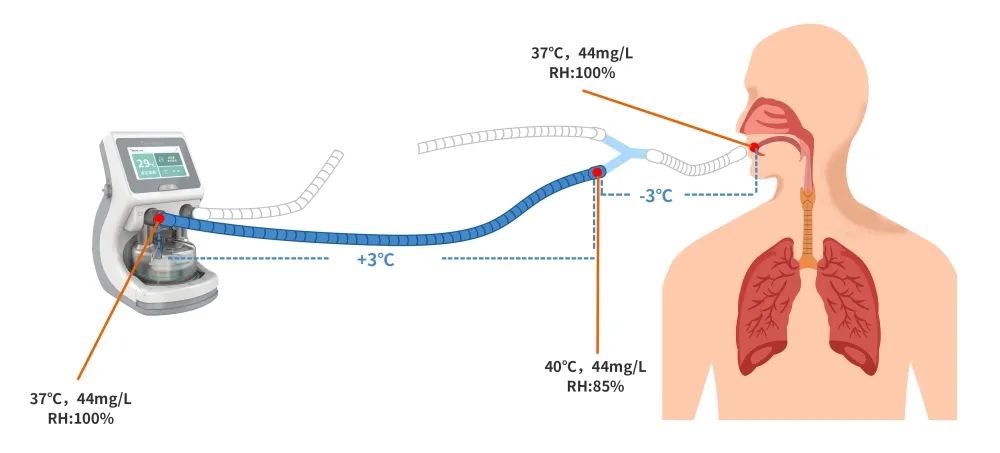
盡管呼吸濕化器可(kě)以保證Y型管處的氣體(tǐ)溫度達到41℃,依據ARRC指南建議Y型管處的最高氣體(tǐ)溫度是37℃,相對濕度是100%。ISO 組織認為(wèi):輸送的氣體(tǐ)溫度持續在41℃以上會對患者帶來潛在的熱損傷,并把43℃作(zuò)為(wèi)熱損傷的高溫報警臨界點。

在進行無創機械通氣時,盡管上呼吸道的生理(lǐ)濕化功能(néng)保留,由于漏氣通氣的特點,單位時間内經過連接界面處的氣流加大,使得患者上呼吸道水分(fēn)丢失,導緻上呼吸道濕化的負荷加重,黏膜濕度不足。此時,使用(yòng)呼吸濕化器可(kě)顯著提升吸入氣體(tǐ)的溫度及濕度,增加患者的依從性和舒适度,從而提高無創通氣的成功率。

1. Lellouche F, Maggiore SM, Lyazidi A, Deye N, Taille S, Brochard L. Water content of delivered gases during non-invasive ventilation in healthy subjects. Intensive Care Med 2009;35(6):987-995.
2. Branson RD. Humidification of respired gases during mechanical ventilation: mechanical considerations. Respir Care Clin N Am 2006;12(2):253-261.
3. Holland AE, Denehy L, Buchan CA, Wilson JW. Efficacy of a heated passover humidifier during noninvasive ventilation: a bench study. Respir Care 2007;52(1):38-44.
4 Solomita M, Smaldone GC. Humidification and noninvasive ventilation. Respir Care 2007;52(1):24-25.
5. Chiumello D, Chierichetti M, Tallarini F, Cozzi P, Cressoni M, Polli F, et al. Effect of a heated humidifier during continuous positive airway pressure delivered by a helmet. Crit Care 2008;12(2):R55.
6. Lellouche F, Maggiore SM, Lyazidi A, Deye N, Taille´ S, Brochard L. Water content of delivered gases during non-invasive ventilation in healthy subjects. Intensive Care Med 2009;35(6):987-95.
7. Williams RB. The effects of excessive humidity. Respir Care Clin N Am 1998;4(2):215-228.
8. Kilgour E, Rankin N, Ryan S, Pack R. Mucociliary function deteriorates in the clinical range of inspired air temperature and humidity.Intensive Care Med 2004;30(7):1491-1494.
9.Shelly MP,Lloyd GM,Park GR(1988) A review of the mechanisms and methods of humidification of inspired gases.Intensive Care Med 14:1-9.
10. Shelly MP(1992) Inspired gas conditioning. Respir Care 37:1070-1080.
返回列表
地址遼甯省沈陽市渾南區(qū)金輝街(jiē)10-4号
關注微信公(gōng)衆号 
